Department of
Sociology
Center for
Innovation
Health Care Delivery Systems
In Developed and Developing Countries
Despite the primary focus on science and technology, the Center has always had a deep interest in the problem of how to improve health care delivery systems. For example, Hage was involved in the research and publication of the book State Intervention in Health Care (Hollingsworth, Hage and Hanneman, 1980), which won the prize that year as the best book in comparative public policy from the International Political Science Association. But the Center’s more focused attention in this area started with the arrival of Wilbur Hadden. The Center has advanced on three fronts: the problem of measuring knowledge advances in medical research in developed countries, the problem of measuring health care outcomes anywhere and the special issues of measuring organizational and institutional problems associated with health care delivery in the developing world.
Evaluating the Usefulness of Systematic Coordinated Inter-Organizational Networks (SCIONs) for Public Health
Our study of the creation of a systematic coordinated inter-organizational network in Nicaragua provides a new approach to evaluation, namely how does one evaluate the impact of a network of organizations? What is the vocabulary that one can use to assess their effectiveness? In this study, we measured the following standards:
- How much heath behavior and knowledge change did the network achieve relative to safe motherhood and child survival?
- How much organizational change did the network achieve defined in four ways: learning, adoption, innovation, and adaptation?
- How much reform of the health care delivery system in Nicaragua was achieved (institutional innovation)?
- Where regional sub-networks established (another form of institutional innovation)?
- Was Nicasalud, the systematic coordinated inter-organizational network institutionalized, i.e. did it survive beyond its initial funding?
Generally, evaluation studies might only look at the first standard and not any of the others. Numbers 2, 3, and 4 represent important additions created by an inter-organizational network. Number two is critical because the real issue in saving societies is how much do the organizations providing services alter their strategies and tactics to become more effective. This solves a fundamental object in the world today, getting organizations to be more adaptive. Standards 3 and 4 move to another kind of change, an important one for saving societies, institutional innovation. The importance of regional sub-networks speaks to two other issues, a literature that suggests the overall network is more effective with regional sub-networks and it provides opportunities to customize services more given local circumstances.
To answer these questions required developing an intellectual framework relative to how SCIONs differ from either market coordination or state regulations and thus contributing to the theoretical literature. In particular, some time is spent carefully defining what the word coordination means in the context of an inter-organizational network since it is so different from either market competition or state regulation coordination modes. To describe organizational strategies and tactics for changing human behavior and knowledge also necessitates a general framework. Our solution is to categorize organizational interventions as either investments in physical capital, human capital, or social capital or some combination of these. In each instance, the study illustrates several sub-categories within each investment type. Besides contributing to evaluation research attempting to change human behavior, our study makes an important theoretical contribution by exploring several distinctive definitions of social capital including participation in women’s groups and the presence of health councils/committees in the villages. Finally, conceptional clarity is brought to the topic of organizational change by carefully defining organizational learning, adoption, innovation, and adaptation and then illustrating these ideas with some powerful findings of how organizational change improves the effectiveness of the organization, a critical criterion for evaluating the effectiveness of a SCION.
The book Saving Societies: Systematic Coordinated Inter-Organizational Networks, innovation and equality, which is in press presents the evaluation. Each chapter provides detailed management lecons and contributions to the social science literature.
Measuring Knowledge Advances in Developed Countries
As noted elsewhere on this site, a major concern of the Center’s has been how to evaluate scientific research. Medical research represents a special category. In a white paper commissioned by the Canadian Academy of Health Sciences Hage (2008) proposed 15 indicators the Canadian government could use evaluate the contributions that research was making.
A grant from the National Science Foundation allowed the Center for Innovation to develop a socio-economic cost-benefit approach that measures the value of medical advances in knowledge by examining recent research studies. Just as in industrial research where only one in twenty projects results in a successful product, so too each scientific research project does not make a major discovery. However, when one occurs, it can have dramatic consequences of saving not only lives but being quite cost-effective. A case in point is a staining technique for lymph nodes around a melanoma cancer. We estimated that if this technique were to become standard practice it would save $1.18 billion in the first year alone, which is about 20% of the annual budget of the National Cancer Institute, and 5.9 billion by the end of five years. As one can observe in the attached pdf file on melanoma, some new therapies cost more than the economic savings but would reduce deaths; others are like silver bullets and both save lives and cost less. (See Hage, 2013; Hadden, 2013)
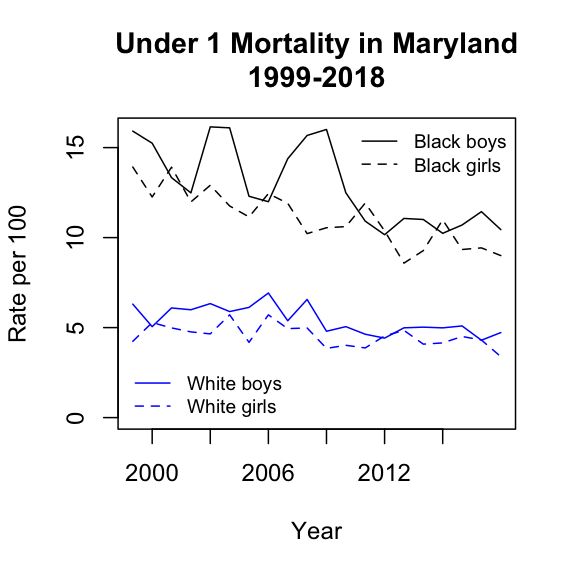
Measuring the Impact of the Affordable Care Act on Infant Mortality in Maryland
The Affordable Care Act was passed and signed into law in March of 2010. The law provided for health insurance exchanges on the internet. The first exchanges, including Maryland's, opened toward the end of 2013. The law required health care plans, beginning in 2014, to cover prenatal and child birth care. Also in 2014 the law supported states in expanding Medicaid, which Maryland chose to do. The figure below suggests that the Affordable Care Act had a positive impact on infant mortality. This appears to be strongest for African-American male infants, but there appear to be improvements for African-American female and for non-Hispanic white male and female infants as well.
Providing Action Theory Solutions for Health Care Delivery in Developing Countries
The Center explored three major problems in providing low cost care in developing countries. The first was to determine if it was better to provide grants to single organizations or multiple organizations. This project took place in Nicaragua. The study found that when multiple organizations were involved, they informally began to develop networks that then put pressure on the Ministry of Health to provide more services to pregnant women during evenings and on weekends. Furthermore, these organizations began to share resources. One of the more interesting findings was the consequences of providing a rooster and a hen to poor families with the proviso that after the birth of the first batch of chicks, they pass the rooster and hen on to another family. This is one way of building social capital at the village level; as each family gives the rooster and hen to the next family, they are building trust and a sense of reciprocity at the village level and sharing experience in food production.
The next project involved a lack of responsiveness in the Indian health bureaucracy to suggestions as to how to improve their use of Lot Quality Assurance Sampling (LQAS). Essentially, the project concluded the root of the problem was that Chief Health Officers at the district level, who make key decisions in this centralized organization, were not cultivated and kept informed about what was happening at the village level (See Hage, Devkota, and Das, 2011).
The third project, in Uganda, posed the question, "Is it possible to institutionalize a LQAS system in such a way that extra funds from international organizations become unnecessary?" Institutionalization was measured by two indices each composed of four components: (1) the degree of training and experience; and (2) the degree of coordination and control of the LQAS process. On the first index, five districts scored 75% or higher and on the second, all but two districts scored this high. Interviews with district health officers and focus groups indicated that LQAS data collection could be integrated into supervisors' and data collectors' on-going work. They also said that they could transfer knowledge to other districts who had not received training. (See Hage, Valadez and Nkolo, 2014).
Measuring the Usefulness of LQAS in Developing Countries
With the cooperation of Joseph Valadez and support from various major international funding agencies, during the past two decades, the Center for Innovation has confronted a number of major issues in how to deliver health services at low cost in developing countries. The monitoring and evaluation part of this effort involves LQAS (See Hage, Devkota, Das, and Valadez, 2011).
A major issue is whether LQAS actually improves the effectiveness of health care services. In the project on Uganda, this was determined in the following way. Two measures of institutionalization were added together and then their rank order correlation at the district level was computed vis-à-vis the percent of mothers having deliveries in a health facility; the Spearman Rho is .45. The causal connection was substantiated with examples from interviews with District Health Officers, Assistant DHO (MCH)s, or their substitutes.
Another project involves examing the factors that impact on responses to feedbacks of information about the relative failure of villages to use malaria nets and to spray to reduce mortality in India. In developing countries, the current technology has been to use LQAS sampling techniques combined with concrete indicators to measure the effectiveness of various interventions to reduce disease and mortality. The first objective of this new project is to explain differences between villages and between districts within the state of Orissa, India, which has the highest rates of malaria in India. The second objective of the project is to develop experiments for testing whether quality work circles composed of villagers and district public health officers can solve problems that are preventing the reduction in mortality from malaria. Theorectically, the project would contribute to the literature on organizational learning by explaining why organizations under certain circumstances do not learn. This project is under the direction of School of Tropical Medicine, University of Liverpool, U.K., which has received World Bank funds to fight malaria.
References
Crossland, N, WC Hadden, WE Vargas, JJ Valadez, and C Jeffery. 2015. "Sexual and Reproductive Health among Ugandan Youth: 2003-04 to 2012." J Adolescent Health 57 (4):393-8. doi: 10.1016/j.jadohealth.2015.06.015. [pdf]
Hadden, W. 2013. Assessing the Benefits of the Colorectal Cancer Program of NCI for the Period of 2006-2008.
[pdf]
Hage, J. 2008. Metrics for the Treatment Scector or Meso Level of the Canadian Health Care System.
White Paper: University of Maryland, Center for Innovation. [pdf]
Hage, J. 2013. Assessing the Benefits of the Melanoma Program of NCI for the Period of 2006-2008.
[pdf]
Hage, J, BR Devkota, and HK Das. 2011. Transforming Public Health Organizations into Learning Organizations: The Case of Malaria Control in Odisha, India
. [pdf]
Hage, J, BR Devkota, HK Das, and Valadez. 2011.Report on the Issues in and Solutions for Organizational Responsiveness to LQAS and Village Acceptance in the Malaria Control Program: A pilot study in the districts of Sundargarh and Kandhamal of the Government of Odisha, India
[pdf]
Hage, J, and JJ Valadez. 2017. Institutionalizing and Sustaining Social Change in Health Systems: The Case of Uganda.
Health Policy and Planning 32 (9):1248-55. doi: 10.1093/heapol/czx066. [pdf]
Hollingsworth, JR, J Hage, and R Hanneman. 1990. State Intervention in Health Care: Consequences for Great Britain, France, Sweden and the United States. Ithaca, NY: Cornell University Press.
Jeffery, C, CA Beckworth, WC Hadden, J Ouma, S Lwanga, and JJ Valadez. 2016. Associations with HIV Testing in Uganda: An Analysis of the Lot Quality Assurance Sampling Database 2003-2012.
AIDS Care 28 (4):519-23. doi: 10.1080/09540121.2015.1112350.
Valadez, JJ, B Devkota, C Jerffery, and WC Hadden. 2019. How Well Do Mothers Recall Their Own and Their Infants’ Perinatal Events? A Two-District Study Using Cross-Sectional Stratified Random Sampling in Bihar, India.
BMJ Open 9:e031289. doi: 10.1136/bmjopen-2019-031289. pdf
Valadez, JJ, J Hage, and W Vargas. 2005. Understanding the Relationship of Maternal Health Behavior Change and Intervention Strategies in a Nicaraguan Ngo Network.
Soc Sci Med 61:1356–68. doi: 10.1016/j.socscimed.2005.02.002. pdf
Updated 10 May 2020
Center for Innovation
Department of Sociology
University of Maryland
College Park MD 20742-1315
Tel: 301-405-6437 Fax: 301-314-6892
UMD Home | Department of Sociology
Maintained by Center for Innovation. Direct questions and comments to webmaster.